Orbital
Anophthalmos
Surgical and prosthetic management of anophthalmos (absence of the eye) and socket reconstruction following enucleation or evisceration.
Medically reviewed by Tamara R. Fountain, MDOculoplastic SurgeonLast updated June 2026
Anophthalmos — Overview
Anophthalmos (or anophthalmia) refers to the absence or loss of the eye within the orbit. The term covers a broad spectrum — from congenital absence of the globe, to acquired loss of the eye from trauma, tumor, or advanced ocular disease. Regardless of cause, the result is an empty or shrunken socket that requires reconstruction to restore volume, support a prosthesis, and maintain a natural facial appearance.
Modern orbital implants and socket-reconstruction techniques have transformed outcomes for patients with anophthalmos. ASOPRS-trained oculoplastic surgeons provide orbital implant surgery, socket reconstruction, and long-term prosthetic management for patients of all ages — including children with congenital conditions who need stimulation of orbital growth.
Classifications of Anophthalmos
Congenital anophthalmos is classified by the stage at which ocular development failed:
- Primary anophthalmia — complete absence of eye tissue from failure of the optic vesicle to develop as an outgrowth of the forebrain neuroectoderm.
- Secondary anophthalmia — the eye begins to develop but stops at an early stage, leaving only residual ocular tissue.
- Degenerative anophthalmia — a partially formed eye regresses, often from a disruption in blood supply during fetal development.
True primary anophthalmos is very rare; extreme microphthalmos (a very small globe within the orbital soft tissue) is more commonly encountered clinically. Anophthalmos and microphthalmos can occur as isolated findings or as part of syndromes associated with chromosomal abnormalities, including Trisomy 13.
Causes of Anophthalmos
Congenital anophthalmos may result from inherited or sporadic genetic mutations, chromosome abnormalities, prenatal environmental insults (infections, teratogens), or unknown causes. Development of the eyelids, conjunctival fornices, and bony orbit depends on the presence of a normal-sized eye during fetal growth; absence or severe reduction of the globe impairs orbital development and requires early intervention.
Acquired anophthalmos results from surgical removal of the eye for trauma (severe injury not amenable to repair), tumor (retinoblastoma, choroidal melanoma, other intraocular malignancies), infection (endophthalmitis unresponsive to treatment), or advanced ocular disease (end-stage glaucoma, a painful blind eye).

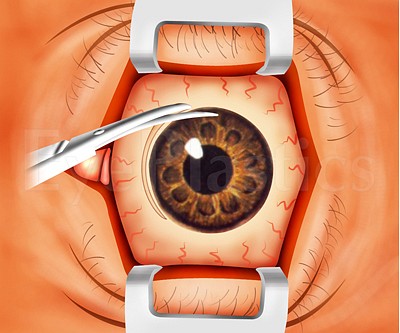
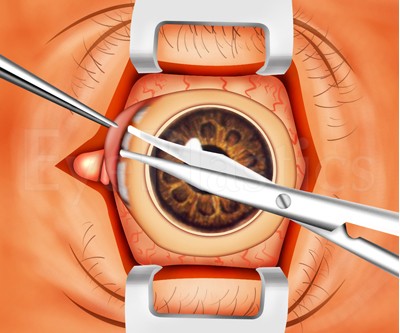
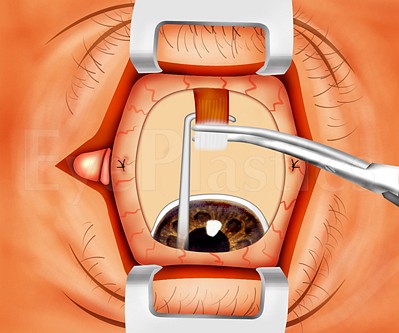
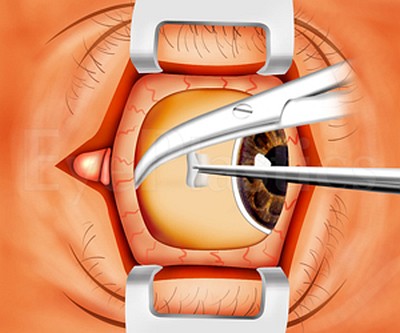
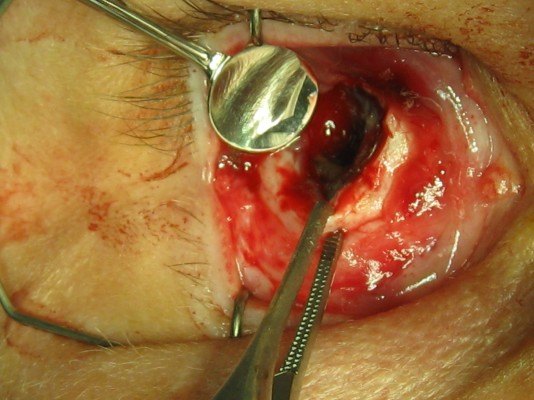
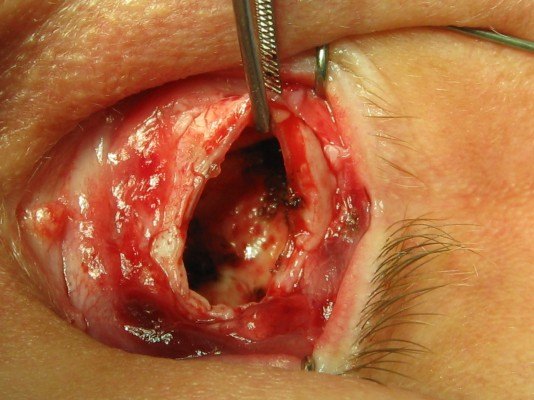
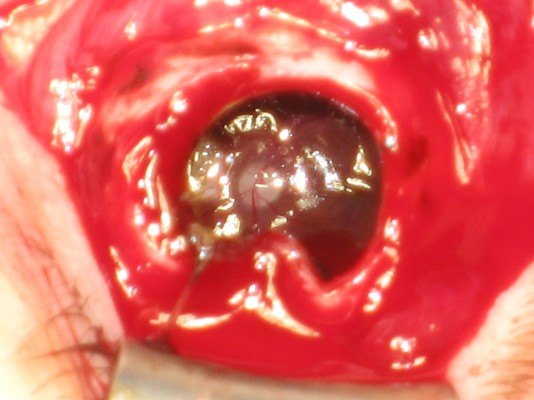
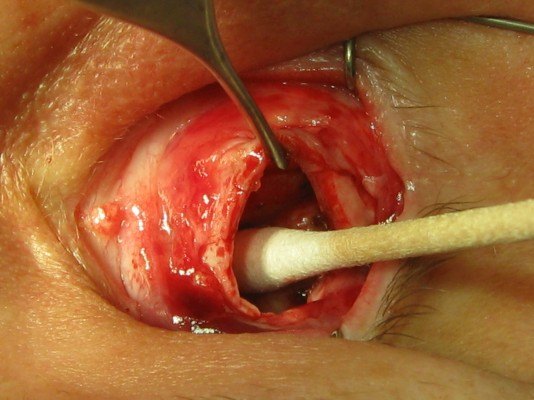
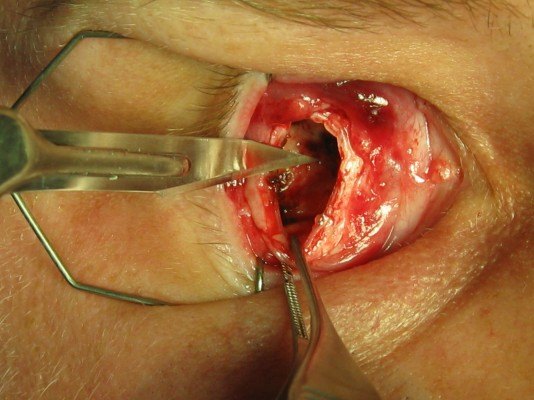
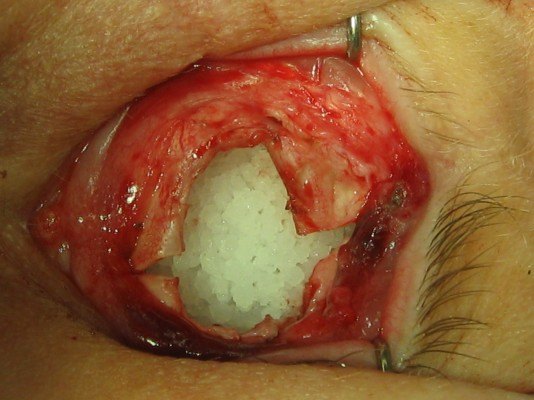
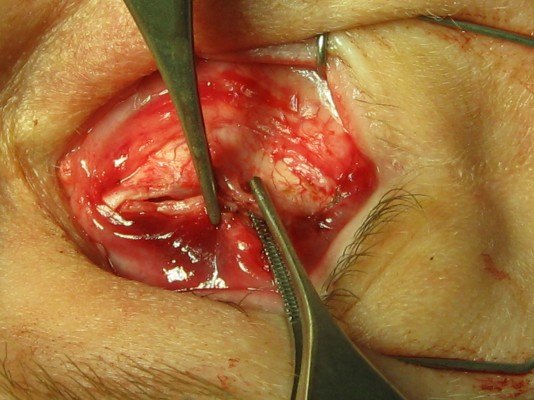
Surgical Options — Evisceration, Enucleation & Exenteration
When the eye cannot be saved, two primary procedures are available:
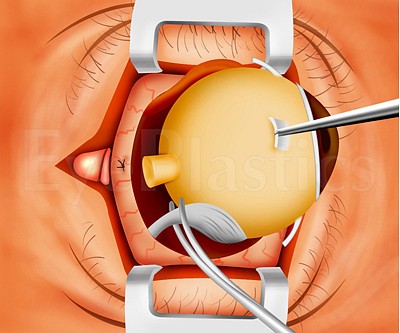
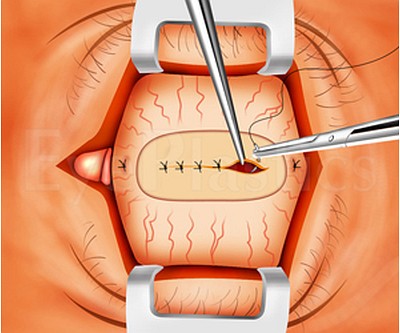
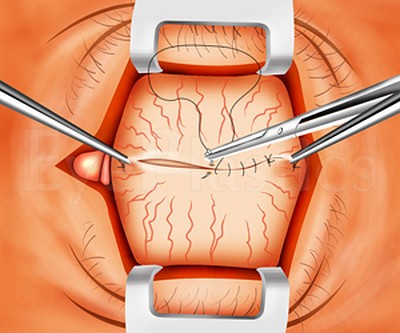
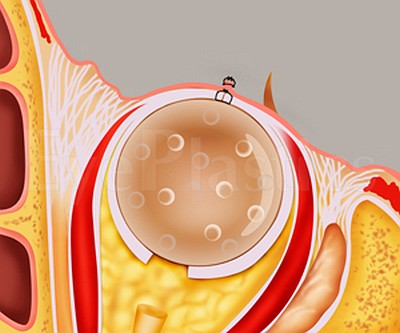
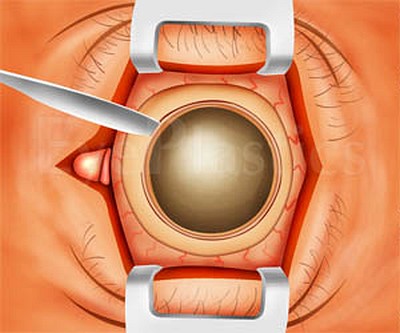
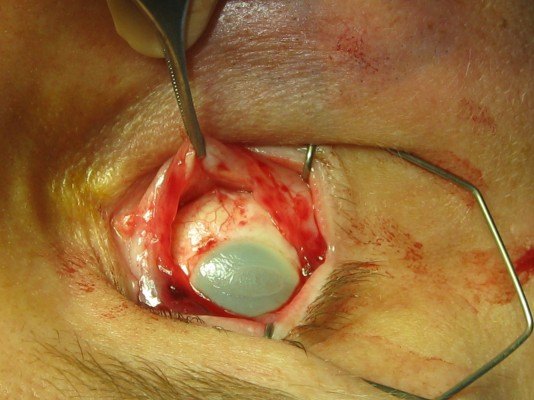
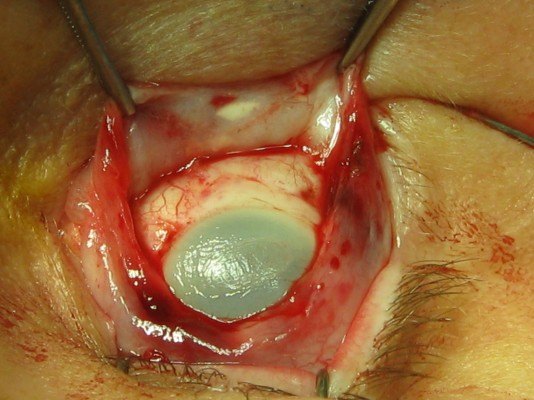
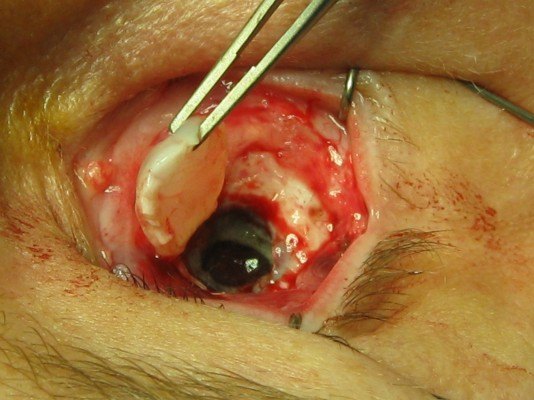
- Evisceration — removal of the intraocular contents while preserving the scleral shell. The sclera and extraocular muscles remain intact, which provides excellent implant motility. Evisceration is generally preferred when there is no concern for intraocular malignancy, as it preserves more tissue and often improves prosthetic movement. It carries a small theoretical risk of sympathetic ophthalmia, though this risk is rare and its comparison with enucleation remains debated.
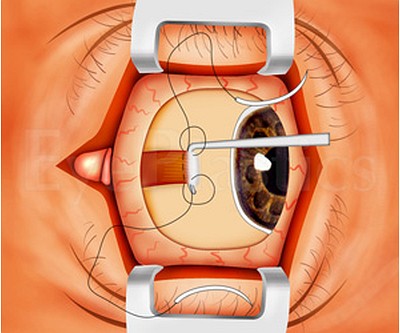
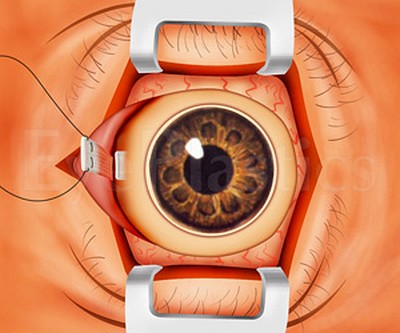
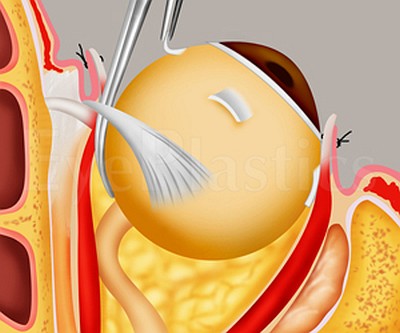
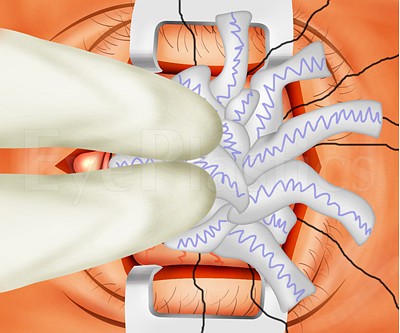
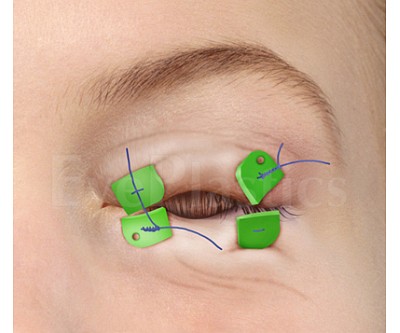
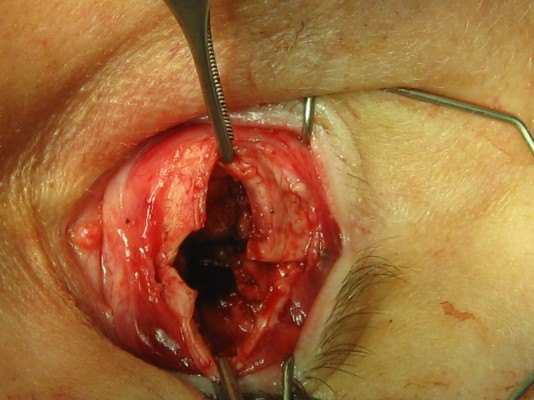
- Enucleation — removal of the entire globe, including the sclera, leaving the extraocular muscles and orbital fat. Enucleation is required when intraocular malignancy is present or suspected. The extraocular muscles are then sutured to the orbital implant to restore movement.
- Exenteration — removal of the entire orbital contents (the eye, orbital fat and muscles, and sometimes the eyelids). It is the most radical option, reserved for life- or sight-threatening disease that has invaded the orbit — most often an aggressive orbital or eyelid malignancy, or an invasive infection such as mucormycosis. The resulting cavity is reconstructed with a skin graft or flap, or rehabilitated with an orbital (facial) prosthesis rather than a standard ocular prosthesis.
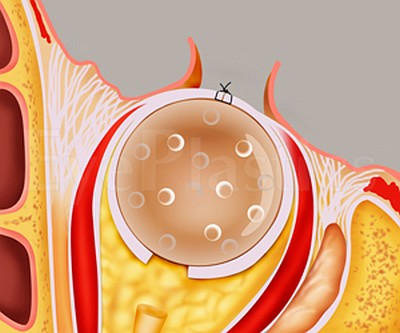
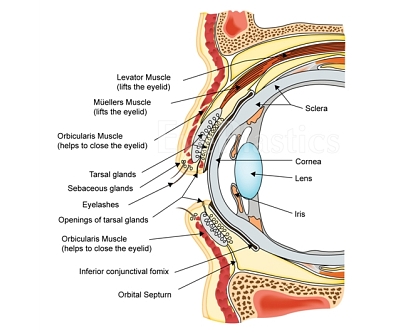
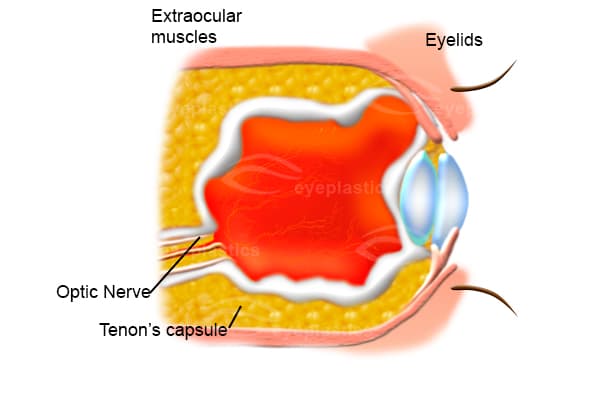
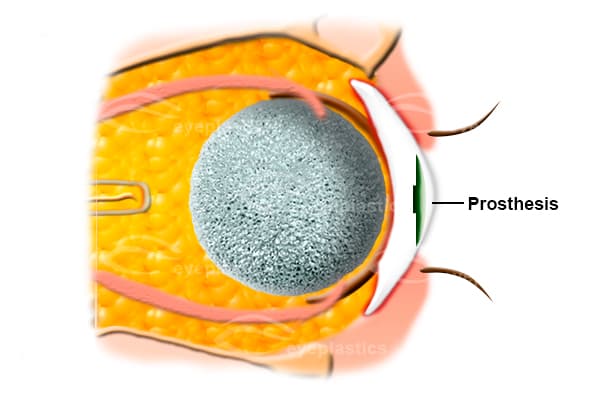
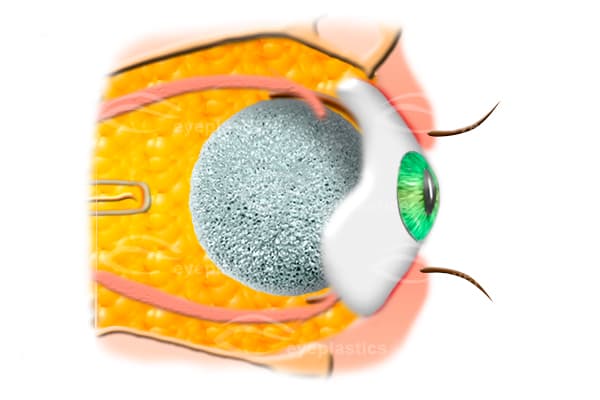
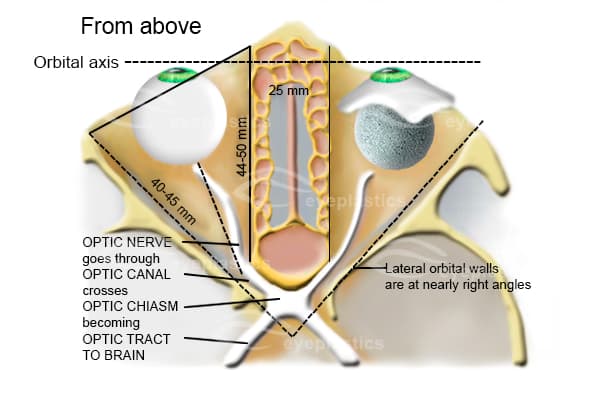
Following either procedure, an orbital implant is placed within the muscle cone to restore orbital volume, and a custom ocular prosthesis is fitted by an ocularist 4–6 weeks later. The animations below illustrate the relevant anatomy and both procedures step by step.
Ready to discuss Anophthalmos?
Schedule a consultation with Tamara R. Fountain, MD to learn if this procedure is right for you.